Download
Status Epilepticus Protocol
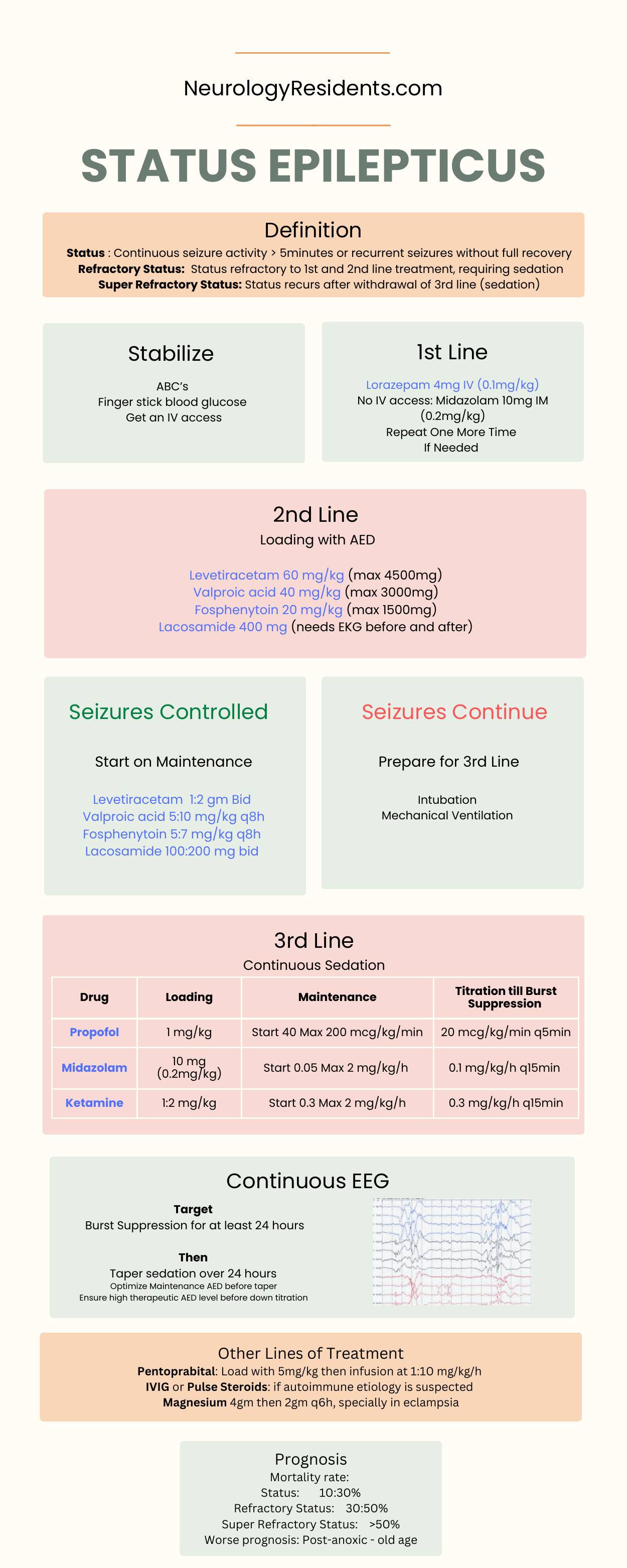
Printable protocol sheet for bedside use.
NeuroResidents
Printable protocol sheet for bedside use.
Status Epilepticus ProtocolStep by step approach Impression: Status Epilepticus: Semiology: *** Etiology: *** PTA AED: *** Plan: Neurological: - Neurological checks q1h - Seizure, fall, aspiration precautions - SBP goal 100-140 - CTH: - Continous video EEG ordered - Burst Suppression: Midazolam drip starting with 0.05mg/kg/h up to 2mg/kg/h till burst suppression is achieved Will continue burst suppression for at least 24h after last seizure (clinical or electrophysiological) Once burst suppression is completed, will taper down sedation over 24h. - Meds: Midazolam drip (starting at 0.05 mg/kg/h, titrate up to 2 mg/kg/h) Propofol at *** mcg/kg/h Continue on home AED medications (***) ___________________ Respiratory: - On mechanical ventilation, mode *** - Daily CXR while intubated - Suctioning q1-2 hours - Meds: - Duonebs q4h _______________________________________________ Cardiology: - Continuous cardiac telemetry - SBP goal 100-140 - Meds: Labetalol 10mg IV q4h prn ________________________________________________ Renal: - Renal function normal - Monitor daily BMP, Mg, Phos - Foley with temperature probe for strict I&O monitoring in critical care setting - Avoid hypotonic fluids as this can worsen cerebral edema - Meds: IVFs with NS at 75/h _______________________________________________ Gastrointestinal: - NPO - Place Dobhoff tube for medication/nutrition; Abdominal X-ray to confirm placement ordered - Start tube feeding with *** @ 10cc/hr and titrate to goal 50cc/hr as tolerated - Hold TF for residuals > 300 - Last BM: unknown - Meds: Docusate 100 mg PO TID Pantoprazole 40mg tab ________________________________________________ Endocrinology: - FSBS q6hr while NPO/TF - Check HgbA1c, TSH - Meds: Insulin SS Hypoglycemia protocol ________________________________________________ Hematology: - Monitor CBC daily - SCDs, enoxaparin 40mg daily for prophylaxis - Meds: - Enoxaparin 40mg q24h ________________________________________________ Infectious Disease: - Current access: PIVs (placed) - Keep normothermic, aggressive fever control as this worsens neurological outcomes - Meds: -APAP 500mg q6h prn fever > 38.3 _______________________________________________ Prophylaxis: DVT: SCDs, enoxaparin 40mg daily GI: pantoprazole, docusate ________________________________________________ Consults: Nutrition ________________________________________________ Discharge Planning: Patient requires ICU level of care for monitoring while on mechanical ventilation. Patient was discussed with the neurocritical care attending who agrees with current plan of management.
Use these templates as educational starting points. Adapt to the patient, the attending, and local policy. Do not place PHI into the public text editor or email workflow.